 An official website of the United States government
An official website of the United States government
 ) or https:// means you've safely connected to the .mil website. Share sensitive information only on official, secure websites.
) or https:// means you've safely connected to the .mil website. Share sensitive information only on official, secure websites.
USAISR Physician Assists in Producing Life-Saving Infusion Tubing
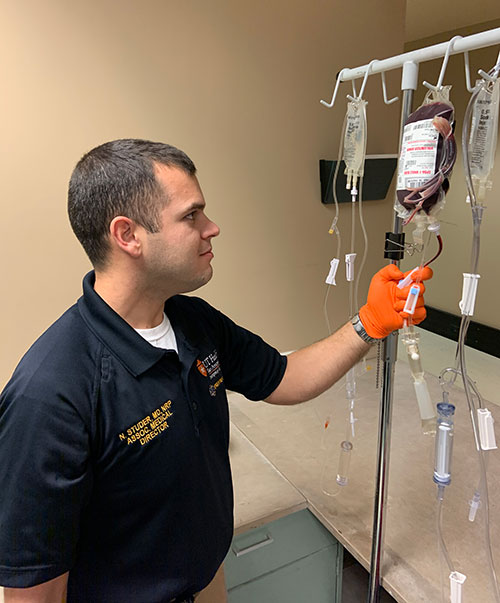
Wounded Warriors injured on the battlefield often require life-saving rapid infusions of blood products shortly after a serious injury. The standard intravenous tubing used for these infusions can constrict the flow of resuscitating fluids, lengthening the amount of time when time is of the essence. As an emergency medical services (EMS) physician, Maj. (Dr.) Nicholas Studer, also a combat casualty care scientist at the U.S. Army Institute of Surgical Research at Joint Base San Antonio-Fort Sam Houston, Texas, understands the urgency of a rapid infusion for critically injured patients and wanted to do something about it.
According to Studer, "trauma tubing" for rapid fluid infusions has existed since the mid-1980s. Physicians modified the tubing used to infuse fluid through the hollow tube (called the cystoscope) used by urologists to examine the urethra and bladder as it was a larger diameter than usual IV tubing.
"Most of these products were discontinued in the 1990s and 2000s as large-volume crystalloid resuscitation went out of favor and hospitals had access to large rapid infuser/warmer products," said Studer.
In 2019, Studer began working with the last producer of "trauma tubing" and modified the "TraumaFlow" product to meet Army and San Antonio Fire Department requirements for rapid pre-hospital blood infusions. In 2018, the SAFD became one of the first EMS agencies in the country to provide prehospital transfusions of whole blood, and remains a leader in the field.
"The Army/SAFD tubing is designed to support either the civilian and military prehospital environments," Studer added. "This particular product was modified to be capable of use with freeze dried plasma or albumin with a vented ‘spike’ to work with the glass bottles these products generally come in. The other spike is of a large bore to allow the maximal flow of whole blood."
TraumaFlow is large-bore (5.0 mm) internal-diameter infusion tubing similar to other "Y-type" blood tubing – but much bigger. Another feature of the Army/SAFD TraumaFlow tubing is that it has a hand pump to increase flow rate when someone is available to squeeze it. Length and the use of an extension set allow it compatibility with all prehospital fluid warmers, while an administration port will allow paramedics to administer Calcium and Tranexamic Acid.
"You can expect that blood tubing is usually twice as fast at infusing fluid as regular IV tubing, and TraumaFlow is three times as fast as regular blood tubing," Studer said.
TraumaFlow is being used by San Antonio Fire Department paramedics, as well as other emergency service providers in other Texas cities, and has been proven to improve the care of trauma patients receiving blood transfusions before arriving at the hospital.
"SAFD has committed to tubing purchase over the next few years," said Studer. "Army EMS has standardized on it for our installation EMS blood programs, with Fort Hunter Liggett being the first to get it. We‘ve learned other cities and military programs are adopting it."
The TraumaFlow tubing’s life-saving features and affordable costs are proving to make this product useful in the hands of military and civilian emergency medical services personnel.
Said Studer, "TraumaFlow is more compact and significantly less costly compared to several other products available to rapidly transfuse blood on the battlefield or in city streets in America."